

Sub-Total: $0.00

Clinician Substance Use in a Treatment Setting: Unexpected Findings from a Facility-Based Study
Theme: Using surveys to explore quality of life in a substance abuse treatment facility
Introduction
Substance abuse research has traditionally centered on clients receiving treatment, with comparatively little attention given to the well-being of the clinicians providing care. In a
recent study I conducted as the principal researcher at a substance abuse treatment facility, findings revealed a surprising and concerning pattern: clinicians reported higher levels of substance use than the clients they were treating. This post summarizes the study’s design, results, and broader implications for the field.
Study Objectives
The primary goal of this research was to examine the quality of life for clients and practitioners in a non-profit substance abuse treatment facility. My aim was to gain a deeper insight into the quality of life experienced by both practitioners and clients receiving substance use or abuse treatment within a specific non-profit organization. By collecting data from both groups, the
study sought to identify not only the patterns of substance use but also the underlying factors that might explain quality of life for those in the study.
Methodology
- Sample: Data collected from two populations within the same treatment facility:
- Clients (n = 19) who were actively engaged in substance abuse treatment.
- Clinicians (n = 14) who provided direct and indirect therapeutic services.
- Instruments: Participants completed the WHO-QOL-100, a valid and reliable instrument used internationally:
- Six quantitative Domains (physical, psychological independence, social, environmental, and spiritual) were the focus.
- Qualitative measurements via qualitative questions overlapped the domains.
- Both clients and clinicians completed the WHO-QOL-100 survey in the Fall and Spring of 2009. The researcher supervised the self-administration of this instrument in an
undisclosed setting to minimize social desirability bias. Comparative statistical techniques were employed to analyze the data, including chi-square tests for categorical variables, t- tests for continuous data, kernel density estimation, regression analysis, and leverage analysis to assess how outliers affect model parameters. Here are a couple of raw visualizations from the data analysis (Box Plots and one of my rvf Plots or
“Leverage”/Residual Plot Analysis.
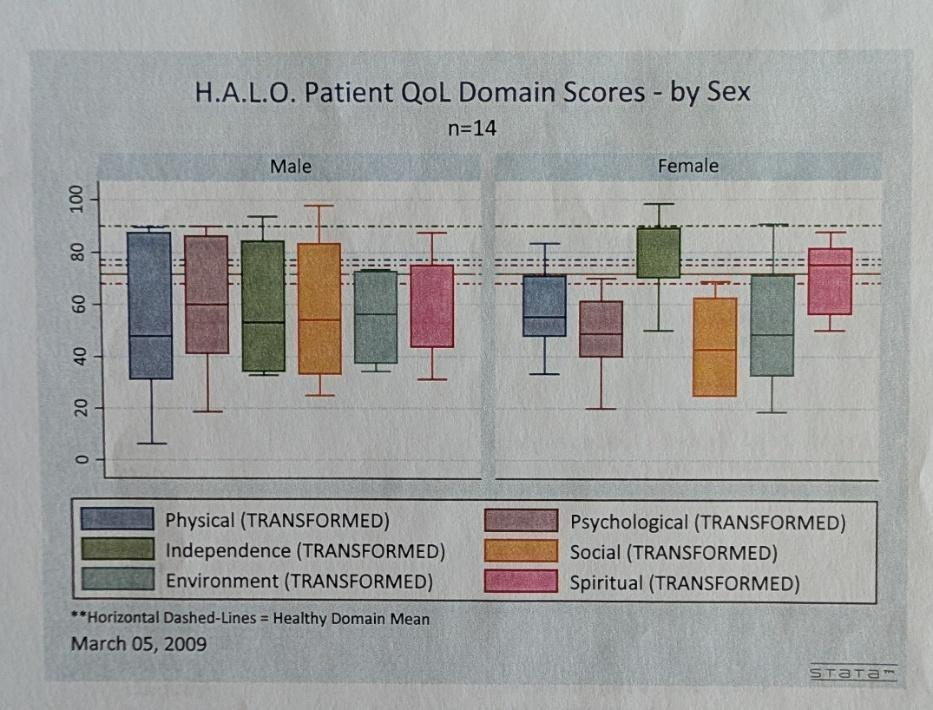
- Box plots from Clinician data with the horizontal lines representing “normal” levels for each of the 6 Domains (Physical, Psychological, Independence, Social, Environmental, Spiritual).
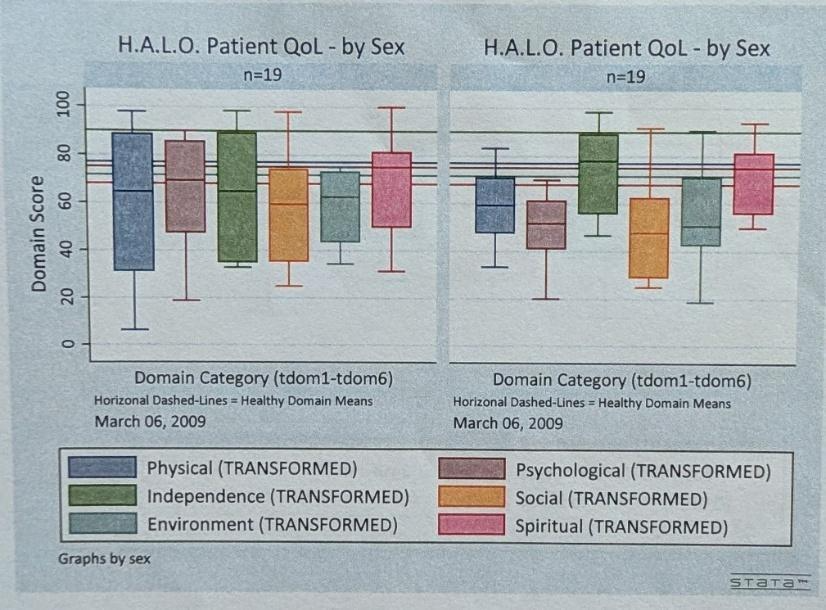
- Box plots from patient data with the horizontal lines representing “normal” levels for each of the 6 Domains (Physical, Psychological, Independence, Social, Environmental, Spiritual).
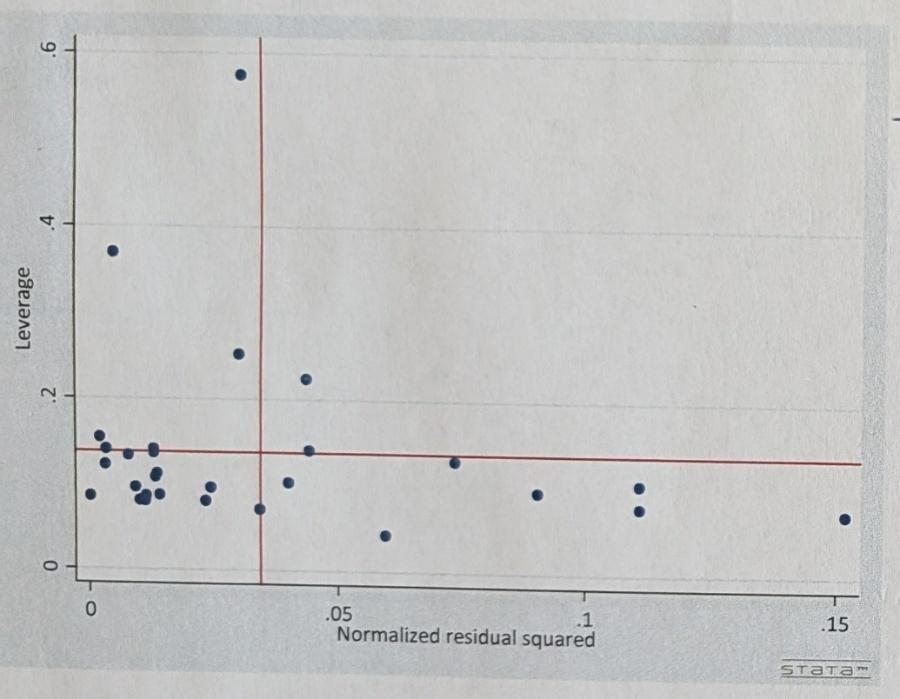
- “Leverage Analysis” (rvf plot) whereby I was looking for dense packing that may allude to “outliers” impacting the model parameter estimates for the Domain regressions.
Below is the regression for Domain #2 (Psychological) on the variables days in
treatment facility (days), age of respondent (age) and marital status (marital). Results here provided me with the ability to justify a deeper analysis of my regression analysis.
Findings
Contrary to expectations, clinicians reported higher levels of substance use and decreased than clients.
- Summary – Quantitative results/findings: from summary statistics to regression
analysis, leverage analysis, the clinicians working directly and indirectly with clients at the treatment facility tended to have equal quality of life for both the WHO-QOL-100 psychological and environmental domains (Domain #2 and #5 respectively) as patients.
In addition, males fared better than females with significantly higher levels of quality of life for these two domains in both clinician and patient populations.
- Summary – Qualitative results/findings: Interviews indicated that clinicians tended to use legal drugs more frequently than they prescribed them to their clients. Although additional research is necessary, these qualitative outcomes are consistent with the study’s quantitative results.
- Barriers to treatment: Clinicians cited stigma, fear of professional consequences, and lack of confidential resources as reasons for not seeking help.
Interpretation
Factors which may help explain these findings:
- Occupational Stress: Clinicians often experience secondary trauma, high caseloads, and emotional exhaustion, which can increase vulnerability to substance use.
- Stigma and Professional Identity: As trained providers, clinicians may feel pressure to maintain a façade of wellness, leading to concealment and underutilization of support resources.
- Normalization of Coping Mechanisms: Easy access and rationalization of use (“I can manage it”) may contribute to elevated prevalence rates.
Implications for Practice
- Organizational Policy: Treatment facilities should integrate clinician wellness programs, including confidential counseling, peer support, and policies that encourage help-
seeking without fear of reprisal.
- Training and Education: Graduate programs and continuing education should include curriculum on clinician self-care, vulnerability, and systemic barriers to treatment.
Future studies across multiple institutions are necessary to determine if this trend occurs in other settings and to find successful interventions.
Conclusion
The study highlights a critical, often overlooked issue in substance abuse treatment: the vulnerability of clinicians themselves and the gender differences in psychological and
environmental quality of life. By recognizing that those who provide care are not immune to the very challenges they diagnose and treat, the field can take meaningful steps toward supporting both client recovery and clinician well-being. The findings call for systemic changes to address stigma, burnout, and access to treatment resources among professionals.